Fat Is Alive
Most people think of fat as being inert, having no real purpose in the body than to keep you warm, and to prevent you from ever having the perfect summer body. The role of fat in the body is so under-appreciated, that when the doctor says, “you need to lose weight”, people often see it as an issue of “body shaming” rather than one of health. This is because fat is not seen as being alive, but as a by-product of too much sugar and starch. While the reality is that fat IS alive, in fact the fat in our bodies is made up of cells called adipocytes, and these cells comprise the functional unit of adipose tissue. Adipocytes and adipose tissue are a part of the endocrine and central nervous system.
Adiocytes – Living Fat
Adipocyte are specialized cells within adipose tissue that contain lipids in the form of multiple round droplets of triglycerides. Triglycerides are the building blocks of fats, as amino acids are the foundation of proteins. Adipocytes simply put are fat cells that transport and produce fat.
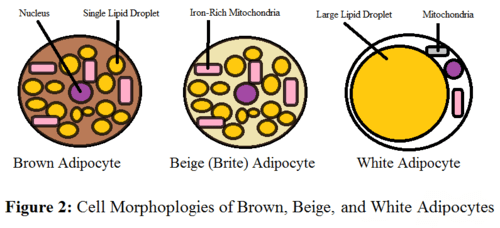
There are three types of fat cells: white, brown, and brown-in-white (“brite”).
White adipocytes are spherical in shape, and are involved in lipid and glucose metabolism. As such they are full of lipid droplets.
Brown adipocytes on the other hand, have fewer goblets of triglycerides than white adipoyctes. Instead brown adipocytes are polygonal in shape and have many mitochondria (mitochrondria are the batteries of the cell). The mitochondria along with a special protein in brown adipocytes called Uncoupling Protein 1 are responsible for heat production, which is facilitated through what’s called, nonshivering thermogenesis. Brown fat is sometimes referred to as good fat, because it burns energy, through generating heat and consumes more energy metabolically, than white fat.
Brown-in-white adipocytes are similar in shape to brown adipocytes but are more functionally akin to white adipocytes, and regulate metabolism and energy.
History
Originally, adipocytes were thought to only serve as storage sites of excess energy; a reservoir for when food intake is low (diet) or when metabolism is high (exercise), and to maintain body temperature. However in the past 50 years scientists have realized a more functional role for adipocytes in the neuro-endocrine system. Fat cells can transmit both neural and chemical signals, making adipose tissue an organ. White adipocytes secrete several chemicals known as adipokines which are involved in inflammation but also paracrine (cell-to -cell) and endocrine signaling, for example adipocytes also have insulin action. In addition to producing chemical messengers, adipocytes receive signals from other tissue and organs in the endocrine system. For instance, brown fat cells are controlled by Leptin ( a hormone produced by white adi
pocytes), and thyroid hormones.
Mechanism of Action
Lipogenesis and Lipid Regulation
White adipocytes can take up glucose, triglycerides, and fatty acids, present in the body from the foods we eat, as well as synthesis their own lipids. When necessary, these sequestered nutrients are secreted back into the blood stream. As such a diet high in carbohydrates and sugars can stimulate lipogenesis or the production of more lipids within adipocytes. Glucose can also cause lipogenesis by triggering insulin secretion from the pancreas.
Neuro-endrocrine Function
Adipocyte neuro-endocrine function is primarily involved in body weight metabolism through regulating the intake of food.
Early mentioned, were adipokines, chemicals secreted by adipocytes that have neuro-endrocrine function. One adipokine in particular, which is involved in studies of weight control and obesity, is Leptin. Leptin is a hormone, a chemical molecule that sends messages to the hypothalamus in the brain, signaling feelings of satiety. Satiation is the feeling of being satisfibly full while eating. Leptin blocks the appetite stimulating neuropeptides that are normally secreted by certain neurons in the hypothalamus. Additionally, Leptin activates Cocaine – and – amphetamine regulated transport neurons that also send messages to suppress appetite.
Leptin regulates appetite, body weight, and fat mass. It is secreted more so by subcutaneous fat, the fat that is right beneath your skin, versus visceral fat. Having a lot of visceral fat, or abdominal fat is associated with increased risk of cardiovascular disease. Additionally, leptin resistance or insensitivity is observed in obesity.
Adiponectin another adipokine secreted by adipocytes, has beneficial functions. It in anti-inflammatory, and is capable of reverseing insulin resistance, which is involved in the pathogenesis of diabetes. Adiponectin is decreased in obsesity, cardiovascular disease, and Insulin-resistant diabetes (type 2), and abdominal fat decreases adiponectin secretion. In addition to being cardioprotective, it also protects renal function, and regulates bone mass.
Imbalances in the ratio of brown fat to white fat could contribute to or be the result of metabolic syndrome/disorders: inflammation, Type 2 diabetes, cardiovascular disease, and even cancer. Having a greater proportion fat versus white fat is healthier. Brown fat helps to prevent many of the above mentioned metabolic disturbances.
Fat wants to maintain its proportions in the body and when increased it releases chemicals to decrease its own mass, such as tumor necrosis factor alpha. This adipokine, formally known as cachexin, causes lipolyis and impairs insulin signaling. Fat cell death results in the release of fatty acids into the bloodstream, but also live adipoctyes are triggered to release their fatty acids in the presence of TNF-alpha. This however, is the case in biologically normal conditions. Under aberrant conditions, adipocytes, particularly white fat cells, adipokine secretion becomes dysregulated and may lead to pathogenesis of cardiovascular disease and other malfunctions of adipocytes known as dyslipidemia.
Adipokines
Adiponectin – anti-inflammatory, anti-artherosclerotic, and renal protective
Leptin- Appetite suppressant action
Cachexin (Tumor necrosis factor alpha) – induces lipolysis (releases fatty acids into blood stream), inhibits insulin signaling
Adipocyte toxicity/pathogenesis
Obesity Is an inflammatory condition and result of metabolic syndrome, the hallmark of which is the major increase in the size of adipose tissue. Generally, obesity is caused by excessive caloric intake coupled with lack of exercise, however other important factors can influence obesity, such as, genetics, endocrine disorders and certain drugs.
Environmental toxins/endocrine disruptors
Environmental toxins known as endocrine disruptors can promote obesity by causing adiocyte toxicity. Polychlorinated Biphenyls (PCBs), like popularly known BPA, can induce adipocyte differentiation, increasing not only their numbers, but also their secretion of pro-inflammatory adipokines. This promotes obesity, which is associated with atherosclerosis.
PCBs are lipophilic compounds, which therefore accumulate in adipose tissue. As such, the amount of PCBs in the body rises with obesity.
Small amounts of PCBs were found to increase the number of adipocytes from precursor cells, while high concentration of BPA were found to decrease adipocyte formation. While high concentration prevented new adipocytes from forming, body weight and fat mass still went up, indicating that existing adipocytes expanded via uptake and storage of increasing amounts of lipids.
Drug induced Adipocyte Toxicity
Highly active anti-retroviral treatment (HAART) used in the management of HIV/AIDS infection can cause adipocyte toxicity, resulting in HIV-associated lipodystrophy syndrome (HALS).
As a side effect of treatment, HAART drugs such as protease inhibitors and non-nucleoside reverse-transcriptase inhibitors, cause adipocyte inflammation, oxidative stress, altered adipocyte function, and mitochondrial damage. These factors cause changes in metabolism and morphology of the body. Metabolically, this means the occurrence of dyslipidaemia, insulin resistance, Type 2 Diabetes, hypertension, endothelial dysfunction, and increased risk of developing cardiovascular disease prematurely. Morphological disfigurement occurs in either the form of abnormal loss or gain of fat in certain parts of the body. Lypodystrophy often presents as fat wasting in the face, limbs, and upper trunk, but also fat accumulation can occur primarily in the back and sides of the neck (buffalo hump) or intra-abdominally.
Protease inhibitor adipocyte toxicity affects cytokine and adipokine production, and results in a decrease in Adiponectin secretion. Protease inhibitors as well as non-nucleoside reverse-transcriptase inhibitors (NNRTI) decrease genes involved in the development of adipoctyes, and NNRTI cause mitochrondria damage by inhibiting mitochrondrial DNA polymerase-gamma.
Summary
Fat is not inert, in fact it is an organ composed of specialized and functional cells called adipoctyes. Adipocytes function in the endocrine system, secreting chemical messengers or hormones, known as adipokines that interact with the central nervous system. Under normal biological conditions, this neuro-endocrine function plays an important role in regulation of body weight and the prevention of cardiovascular disease and diabetes through the suppression of appetite in the case of leptin and anti-inflammatory, antiartherosclerotic, and insulin sensitivity action of Adiponection. However, abnormalities in adipose tissue can arise when energy intake exceeds normal dietary requirements or from exposure to environmental toxins and certain drugs. In this case, imbalances between brown and white fat, as well as increase in fat mass, particularly abdominal fat, results in the decrease of adiponection secretion, leptin insensitivity, and increases in tumor-necrosis factor-alpha and inflammatory adipokines that contribute to atherosclerosis.