
Most people can recall being asked by the doctor whether they have an allergy to penicillin or not. In fact, 10 percent of the general population is estimated to have Penicillin Allergy. However, in the past few years, the prevalence of Penicillin Allergy has decreased.
Studies have found that when tested, the vast majority of people who reported having Penicillin Allergy, are not allergic to the drug. Clinicians found, that many people who were told they were allergic to penicillin, never had their allergy confirmed with testing. Interestingly, others who were positively diagnosed in the past, were no longer allergic to penicillin.
Unverified Penicillin Allergy reports are problematic, and pose a Public Health concern. Patients who are allergic to Penicillin must be treated with alternative antibiotics, that have a broader spectrum of activity. The use of broad-spectrum antibiotics are associated with the development of drug-resistant bacteria. In addition, alternative antibiotics contribute higher costs to both the patient and the healthcare system, due to iatrogenic infections, higher cost for treatment, and longer hospital stays.
Penicillin Allergy
Penicillins are generally safe and have low toxicity, however Penicillin has the ability to cause allergic sensitization. Allergic reactions to Penicillin results from the formation of haptens. Haptens are drug-protein complexes in the body that stimulate an immune response. Penicillin and its metabolites (degradation products) covalently binds to proteins and this complex acts as an antigen. Antibodies are then formed against the antigen, creating a hypersensitivity to subsequent exposures to the drug.
Penicillin Allergies are unpredictable adverse drug reactions. The most common are either immediate (Type I) or delayed (Type IV) hypersensitivity responses. Immediate responses typically occur within an hour, while delayed responses may not present for days or weeks. The most common reaction results from a Type I IgE-mediated (Immunoglobulin E- antibody) response, which causes skin rashes. With the exception of anaphylaxis, less common and more severe hypersensitivity reactions occur from type IV non IgE-mediated immunological responses.
Immediate IgE- Mediated Symptoms
- Urticaria (hives)
- Anaphylaxis
- Angioedema (swelling of lips, tongue, face, and periorbital tissue)
- itching giant hives wheezing
- shortness of breath
- Cardiorespiratory Collapse
- light-headedness
- muscular weakness
- blurred vision
Signs and Symptoms
The most common reaction to penicillins are Maculopapular or urticarial rashes, which are most likely to appear immediately (within an hour or a day). Penicillin allergies also cause, fever, bronchospasm, vasculitis, serum sickness, and exfoliative dermatitis, Steven-Johnson’s Syndrome and Anaphylaxis.
Delayed Non IgE-mediated Symptoms
- maculopapular rash
- hemolytic anemia
- serum sickness
- Stevens-Johnson syndrome
- acute interstitial nephritis
- toxic epidermal necrolysis
An allergic reaction to one penicillin poses the risk of having a greater negative response if given another type of penicillin. Therefore, another class of antibiotic is prescribed for patients who have Penicillin Allergy.
Antibiotics & Penicillin
 Penicillins are the oldest antibiotics, and the drug of choice for the treatment of respiratory tract infections, anaerobic infections, pneumonia, meningitis, syphilis, and gonorrhea. Like other antibiotics they are derived from natural substances produced by microorganisms that retard the growth of other microbes, such as, fungi and other bacteria. As such, Penicillin is derived from the mold/fungi Penicilium Chrysogenum, which was accidentally discovered In 1928, by Alexander Fleming. When he noticed that mold contaminating his cultures inhibited neighboring Staphylococcus bacterial growth, Alexander Fleming grew-up the mold in a broth. Using it, he found that the broth had antibacterial properties.
Penicillins are the oldest antibiotics, and the drug of choice for the treatment of respiratory tract infections, anaerobic infections, pneumonia, meningitis, syphilis, and gonorrhea. Like other antibiotics they are derived from natural substances produced by microorganisms that retard the growth of other microbes, such as, fungi and other bacteria. As such, Penicillin is derived from the mold/fungi Penicilium Chrysogenum, which was accidentally discovered In 1928, by Alexander Fleming. When he noticed that mold contaminating his cultures inhibited neighboring Staphylococcus bacterial growth, Alexander Fleming grew-up the mold in a broth. Using it, he found that the broth had antibacterial properties.
Antibiotics are agents that are used to treat infections by inhibiting or killing bacteria. There are many types of antibiotics, and not all antibiotics function the same way. Therefore, antibiotics are grouped into classes based on their chemical structures and mechanisms of action. In addition, there are synthetic antimicrobials, such as, sulfonamides and quinolones, that are also classed as antibiotics.
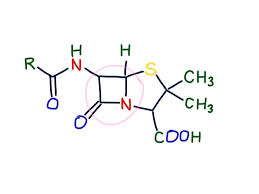
Penicillin and its derivatives, together are termed Penicillins. Penicillins belong to a class of antibiotics known as beta-lactams. They are so termed, because as a group, they can be degraded by an enzyme produced by bacteria, called beta-lactamase.
Beta-Lactams
- Penicillins/aminopenicillins
- Cephalosporins
- Carbapenems
- Monobactams
- Beta-lactamase inhibitors
Mechanism of Action How Penicillin kills bacteria
Beta-lactams kill bacteria by inhibiting the synthesis of peptidoglycan in the cell wall. Peptidoglycan is the component of the cell wall that is responsible for its mechanical rigidity and stability. The cell wall protects the cell-membrane of bacteria guarding against cell lysis.
Peptidoglycan is a heteropolymer made-up of cross-linked glycan chains and peptide chains. Beta-lactams inhibit the synthesis of peptidogycan by interfering with transpeptidase, a cell-membrane bound enzyme responsible for the cross-linking of peptides. Beta-lactams also kill bacteria by interacting with penicillin-binding proteins. Penicillin covalently binds to penicillin-binding proteins and eventually causes cell lysis. Penicillin may also cause non-lytic cell death through interactions with other proteins.
Risk & Exposure
Previous exposure to Penicillins is necessary to develop Penicillin Allergy. All penicillins have the potential to cause an allergic response. Allergenicity does not depend on the dosage or the type of penicillin given. However, there are several factors that can increase the likely hood and severity of an allergic response, should one occur.
The route of administration is one such factor. Parenteral administration of Penicillins (given intravenously) has been shown to cause more severe allergic reactions compared to oral administrations. Another factor that may influence the severity of reaction is Atopy, or a genetic disposition towards developing allergies. Atopy, makes you more reactive to the drug than normal. As such, a history of allergy to other drugs, also poses an increased risk of Penicillin Allergy.
Recent use of a penicillin increases the risk of experiencing an allergy reaction. Most people who are allergic to Penicillin were exposed to the drug through treatment for bacterial infection in the past. However, some people who are allergic, report never haven received Penicillin. Exposure to penicillin, can occur from the environment, as traces of penicillin has been found in small amounts in meat and milk. Residual penicillin in meat and dairy result from the administration of antibiotics to animals, and can cause hypersensitivity in humans.
Age may also play a role, as persons between the ages of 20-49 were found to be more likely to have a true Penicillin Allergy.
Not Allergic to Penicillin Decline in the prevalence of Penicillin Allergy
The prevalence of Penicillin Allergy has declined for various reasons. Firstly, most people who report being allergic to penicillin were misdiagnosed. Some who self-reported an allergy, had been erroneously informed by a parent or incorrectly remember a childhood experience. Others, who were reported by a clinician, had an adverse event — related to their illness—mistaken for an allergic reaction to Penicillin. In most cases, the diagnosis of Penicillin Allergy was never verified with skin testing or oral challenge.
Secondly, having an adverse reaction to penicillin one time, does not guarantee that you will have an allergic response upon subsequent exposure. The reason for this, is that, allergy to penicillin wanes overtime. At least 80% of people who had true immediate IgE-mediated allergic reactions to penicillin, lost their sensitivity to the drug within 10 years.
Changes in the way antibiotics are prescribed have also contributed to the decrease in Penicillin allergies. The use of intravenously administered penicillin and oral amoxicillin were responsible for many penicillin related allergic reactions. Penicillin is rarely given intravenously anymore, and rashes attributed to amoxicillin were found to be complications of underlying infection with Ebstein-barr virus.
Unverified Penicillin Allergy Consequences of Alternative Antibiotic Treatment
Unverified Penicillin Allergy labeling is a Public Health concern. Penicillins are the most frequently prescribed drug. Their low-cost, high safety profile, and bactericidal activity against both gram-positive and gram-negative bacterium make them the antibiotic of choice. However, when Penicillin Allergy is present, treatment with Penicillins is contraindicated. But, most persons labeled as allergic to penicillin are in fact able to tolerate the drug. Yet, they are unnecessarily prescribed alternative antibiotics, because of unverified diagnosis of Penicillin Allergy.
Penicillin Allergy labelled patients are prescribed antibiotics that are more expensive and more toxic. They receive broad-spectrum antibiotics that can be less effective, and carry the risk of developing multi-drug resistant bacteria. In addition, antibiotics prescribed in lieu of Penicillins often lead to the development of iatrogenic infections, such as, clostridium difficile or candidiasis. The healthcare system also carries the burden of cost. Patients deemed allergic to Penicillins are admitted into the hospital for longer stays, with more extensive treatments, due to the price of drugs and the management of iatrogenic infections.
Penicillin Allergy Testing
In order to verify Penicillin Allergy, skin testing or oral graded-dose challenge are recommended to be performed when the likelihood of true Penicillin Allergy is suspected to be low. Patients previously labelled as allergic to Penicillin, who test negative, can be administered Penicillins.
Only suspected non allergy to Penicillins caused by immediate IgE-mediated hypersensitivity reactions should be tested, as anaphylaxis to even very small amounts of skin prick doses can occur. Furthermore, delayed, non IgE-mediated Penicillin Allergy patients should never be subjected to skin testing, graded-dose challenge, or desensitization. Desensitization should only be carried out in cases when true IgE-mediated Penicillin Allergy exists, but treatment with beta-lactam antibiotics is absolutely required.
Summary
In the United States about 10% of people are reported to have Penicillin Allergy. However, improved clinical practices have revealed that 80 to 90 % of these people are actually able to tolerate treatment with Penicillin. They were either never allergic to Penicillin or lost their sensitivity to the class of drug, overtime.
Over estimation of Penicillin Allergy has led to the use of alternative broad-spectrum antibiotics. Broad-spectrum antibiotics are generally more expensive, more toxic, and less effective. As a result, patients and hospitals incur more costs. Broad-spectrum antibiotic are linked to higher rates of antibiotic resistance, longer hospital stays, and patients treated with these drugs, often develop iatrogenic infections, such as, Clostridium difficile.
Confirming true Penicillin Allergy reduces the inappropriate use of second-choice broad-spectrum antibiotics, and reduces the development of multidrug-resistant bacteria. It saves money and reduces recovery time in patients.

Yes, yes and yes! People tend to say right off the bat that they have a penicillin allergy yet has either taken it a long time ago or if at all. It makes it very difficult to administer it especially when other antibiotics can cost almost $1500 a day. As a nurse, I try to clarify if the person really has an adverse reaction to it. But in this customer service-based healthcare system of ours…plus Wikipedia…people do not want the cheap stuff.
LikeLike
I find that people become aware that something can cause an allergy, and they just assume that means that all people are allergic to it…I see this happening with gluten.
LikeLike